

The first clinical study using EOlife in a blinded mode conducted by the Paris Fire Brigade (BSPP) highlights the urgent need to improve manual ventilation quality during CPR.
This study included 104 adult patients who suffered out-of-hospital cardiac arrest (OHCA) and examined the quality of manual ventilation provided by the professional firefighters of the brigade during CPR. These highly trained emergency responders are among the most skilled in prehospital care, serving as a reference for other fire and rescue services in France. Throughout the study, key ventilation parameters—including tidal volume (Vt), insufflated volume (Vi), and leakage rate—were recorded using EOlife. The device was used in a “blinded” mode, capturing ventilation data without providing feedback to the users, allowing them to ventilate as they normally would.

EOlife, the only Ventilation Feedback Device (VFD) to display the volume of gas reaching the patient’s lungs (Tidal Volume).
CE-marked and FDA-cleared medical device enabling real-time measurement of insufflated volume, tidal volume, and ventilation frequency. It provides visual feedback to deliver ventilation following ERC or AHA recommendations.
A significant gap between guidelines and clinical practice
The study results reveal a substantial discrepancy between international recommendations and real-world clinical practice. While the median insufflated volume (538 mL) aligns with guidelines, it exhibits significant variability [412–645 mL]. More concerning is the consistently high leakage rate observed throughout resuscitation (41%, equivalent to 199 mL), resulting in a median delivered tidal volume of only 291 mL—well below recommended levels.
Recent research demonstrates that such low tidal volumes severely compromise patient survival chances and neurological recovery. These findings underscore the urgent need to enhance ventilation quality and integrate real-time feedback devices like EOlife, even within elite emergency response teams.
Unexpected differences between the two insufflations
A closer analysis of the results, as shown in the figure below, reveals a surprising pattern. The leakage ratio for the first insufflation is significantly higher than for the second. Several hypotheses could explain this phenomenon:
- Airway closure due to chest compressions
Chest compressions may progressively close the airways, increasing overall respiratory resistance. As a result, the first insufflation encounters greater resistance, leading to a higher peak pressure and an increased leakage rate. Once the airways are opened by the first insufflation, the second may be more effective.
- Air trapping due to insufficient expiration time
Given the very short time available for ventilation in 30:2 CPR, the second insufflation may sometimes occur before full exhalation of the first breath. This could lead to “air trapping,” where residual air remains in the lungs, reducing the volume expired during the first ventilation.
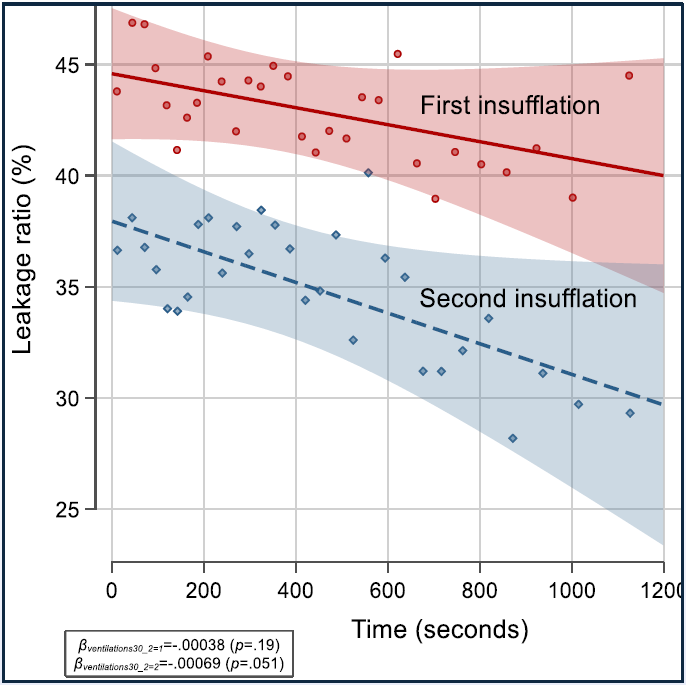
Leakage rate decreases over time: evidence of improved mask positioning?
Another interesting observation is that the leakage rate appears to decline as resuscitation progresses. This suggests that firefighters may gradually refine their mask positioning, leading to more effective ventilation.
This first clinical study using EOlife highlights a critical gap between international guidelines and real-world CPR practices. High leakage rates result in extremely low tidal volumes, with unexpected variations between the first and second ventilations. These findings emphasize the urgent need to improve manual ventilation quality and implement real-time monitoring and feedback systems like EOlife.
Stay ahead in CPR research and learn more about EOlife Ventilation Feedback devices
Find out more
References
(1) Evaluation of ventilation quality of BLS Firefighter teams during OHCA : The VECARS – 1 study. F. Lemoine, D. Jost, B Tassart, A. Petermann, S. Lemoine, M. Salome, B. Frattini, S. Travers.