

Over the last decade, CPR training has been transformed by feedback technologies. Compression depth, recoil, rate, and hands-off time are now objectively measured and continuously optimized during training sessions. As a result, chest compression quality has become measurable, reproducible, and easier to improve.
Ventilation, however, remains the forgotten component of resuscitation education.
Despite overwhelming evidence showing that hyperventilation and poor tidal volume delivery negatively impact patient outcomes, ventilation training is still largely based on subjective observation, like watching for chest rise.
If ventilation truly matters during cardiac arrest, then it must be taught with the same rigor as chest compressions. It must become measurable, quantifiable, and objectively assessed.
> Watch the video
The invisible gap, why subjective training is no longer enough
Ventilation feedback devices (VFDs) such as EOlife X represent a major step forward in CPR education. By providing real-time measurements of tidal volume, ventilation rate, leakage, and overall ventilation quality, they transform ventilation from an approximate manual skill into an objective clinical parameter.
But recent evidence suggests a deeper issue: ventilation feedback devices are not just improving CPR training. They are exposing the hidden limitations of CPR manikins themselves.
How feedback devices expose flaws in CPR simulation
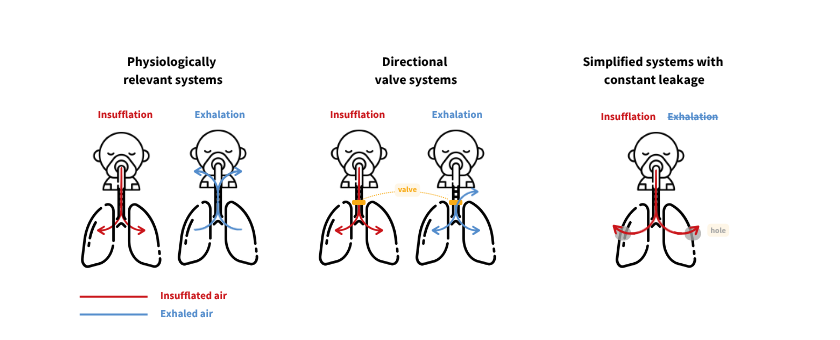
A recent bench evaluation of ten widely used adult CPR manikins (1) demonstrated major variability in the way ventilation is simulated. The study identified three main categories of respiratory systems:
- Physiologically relevant systems, allowing inhalation and exhalation through the airway.
- Directional valve systems, preventing expiratory airflow from returning through the airway.
- Simplified systems with constant leakage primarily designed for basic instruction.
These differences are far from anecdotal. They determine whether ventilation can actually be measured correctly. Because feedback devices rely on physiological airflow signals, a manikin without measurable expiratory flow makes objective evaluation of tidal volume nearly impossible.
The takeway: When ventilation measurements appear inconsistent, the issue may not come from the feedback device itself, but from the inability of certain manikins to reproduce realistic respiratory physiology.
In many ways, feedback devices are acting as revelators. They expose limitations that previously remained invisible because ventilation quality was never objectively measured in the first place.
Why Objective feedback fundamentally changes ventilation training
One of the greatest strengths of ventilation feedback devices is their ability to immediately identify inadequate ventilation behaviors that traditionally go unnoticed during CPR training, such as:
- Excessive or low ventilation rates.
- Insufficient or excessive tidal volumes.
- Poor mask sealing.
Real-time correlation
Instead of relying on subjective impressions, clinicians can immediately correlate their actions with measurable physiological consequences. They can see when ventilation becomes excessive, when leakage occurs, or when delivered volumes fall outside recommended targets.
This creates a much more effective educational environment. Learning becomes faster, more reproducible, and more consistent between providers.
Ventilation should not remain the last blind spot of CPR training quality improvement.
When poor manikin design undermine clinical training
The same study also highlighted another critical issue: significant air leakage across many CPR manikins, including when supraglottic airways or endotracheal tubes were correctly positioned.
The implications for training are substantial.
VFDs are specifically designed to detect leakage and guide providers toward optimal ventilation techniques. However, when leakage originates from the manikin itself rather than from the operator, learners receive misleading feedback.
Over time, this can normalize poor ventilation behaviors instead of correcting them.
Without objective feedback, these problems remain hidden. With VFDs, they become immediately visible.
This is precisely why ventilation feedback technologies should not be viewed as optional educational accessories. They are becoming quality control systems for CPR training itself, capable not only of improving learner performance, but also of identifying limitations within the training environment.
The future of CPR training requires ventilation feedback
High-quality CPR education requires two inseparable components:
- physiologically realistic simulation
- objective ventilation feedback.
One without the other is insufficient. A realistic manikin without feedback cannot quantify performance, while a feedback device used in a non-physiological simulation environment cannot generate clinically meaningful data.
Together, however, they create something CPR training has historically lacked: measurable ventilation quality.
Ventilation feedback devices such as EOlife X should therefore become the standard in advanced CPR training. We must ensure that training conditions accurately reflect respiratory physiology encountered in real patients.
After all, clinicians do not ventilate manikins in real life: they ventilate patients.
Ready to upgrade your training standards?
And you? Is your training equipment giving you the full picture or just a reflection of its own limitations? [Book a demo] and discover how EOlife X is setting a new standard for objective ventilation.

(1) Urkarthofer D, Weldi M, Trathnigg G, Billig S. Ventilation characteristics of cardiopulmonary resuscitation manikins: a mixed-methods bench study. Resuscitation Plus. 2026;101318. doi:10.1016/j.resplu.2026.101318
https://www.sciencedirect.com/science/article/pii/S2666520426001037