

New evidence from Bob Page’s JEMS interview

Is your manual ventilation based on data or just a “gut feeling”? For decades, the Bag-Valve-Mask (BVM) has been the gold standard for resuscitation, yet it remains one of the most inconsistently performed skills in emergency medicine.
In a groundbreaking article recently published in JEMS, Bob Page (founder of the Manual Ventilation Academy) reveals the results of a 15-month study involving over 30,000 recorded ventilations. The conclusion is clear: without real-time feedback, even the most experienced providers struggle to meet clinical guidelines.
Why real-time feedback is essential for proper manual ventilation?
Traditionally, competency in BVM ventilation has been assessed using subjective markers:
– visual chest rise
– provider confidence
– instructor observation
However, manual ventilation is a quantitative physiological intervention. It is defined by two critical variables that the human eye cannot accurately measure:
Tidal Volume (Vt): The volume of gas delivered per breath.
Ventilation Rate (Fr): The number of breaths per minute.
Without real-time measurement, manual ventilation is an “unmeasured intervention,” relying on estimation rather than controlled clinical delivery.
Historical training limitations
In an article recently published in JEMS, Bob Page, from the Manual Ventilation Academy, an entity dedicated to training healthcare providers in High-Performance Ventilation, describes early training paradigms where BVM ventilation was taught through repetition, instructor feedback, and visual assessment of chest rise. Competency was assumed rather than measured.
This limitation persisted even with the introduction of simulation technology. Even with advanced simulation technology like the ASL 5000 (Ingmar), learners often only see their performance after the scenario is over. As a result, learning remained iterative and inefficient, requiring repeated attempts before performance improved.
This highlighted a critical educational gap: measurement without point-of-care feedback does not change behavior in real time.
The feedback hypothesis
The Manual Ventilation Academy set out to prove a simple but bold theory:
“If learners receive real-time, breath-by-breath physiological feedback, their accuracy and consistency will significantly improve compared to blinded ventilation.”
This hypothesis led to the development of structured feedback-based training and research programs starting in 2024.
The study: 2,000 participants, +30,000 breaths
Between 2024 and 2025, a massive simulation-based research program was conducted across 28 U.S. states, Canada, and the UK. Using EOlife X to collect data in both “blinded” and “feedback” modes, the study analyzed 33,887 breaths.
All participants underwent standardized ventilation scenarios using standard BVMs, identical manikin platforms, and controlled airway conditions. EOlife X was used, in blind and feedback modes, to collect ventilation data and guide users during the feedback phase.
Study design
Participants performed manual ventilation under three controlled conditions:
1. Blinded ventilation: no real-time feedback from EOlife X.
2. Feedback familiarization phase: short exposure to the real-time feedback of EOlife X.
3. Feedback-enabled ventilation: ventilation using the real-time feedback from EOlife X.
Each participants ventilated for two-minutes interval in each conditions.
The results: data vs. estimation
These results demonstrate a statistically significant improvement in mean tidal volume, a statistically significant reduction in variability, and improved consistency around guideline-recommended ranges when feedback is used:
Without feedback: 293.83mL mean Vt ; p<0,05
With EOlife’s feedback: 436.43mL mean Vt ; p<0,05
They highlight how poorly rescuers ventilate without real-time feedback, and how dramatically EOlife X improves guideline adherence.
Device-independent findings
To confirm these findings across multiple ventilation settings, Bob Page conducted a comparative study with various ventilation devices (Sotair Safe BVM, Pulmodyne VT Select, and standard adult BVM AMBU SPUR II as the control group). The results are as follows.
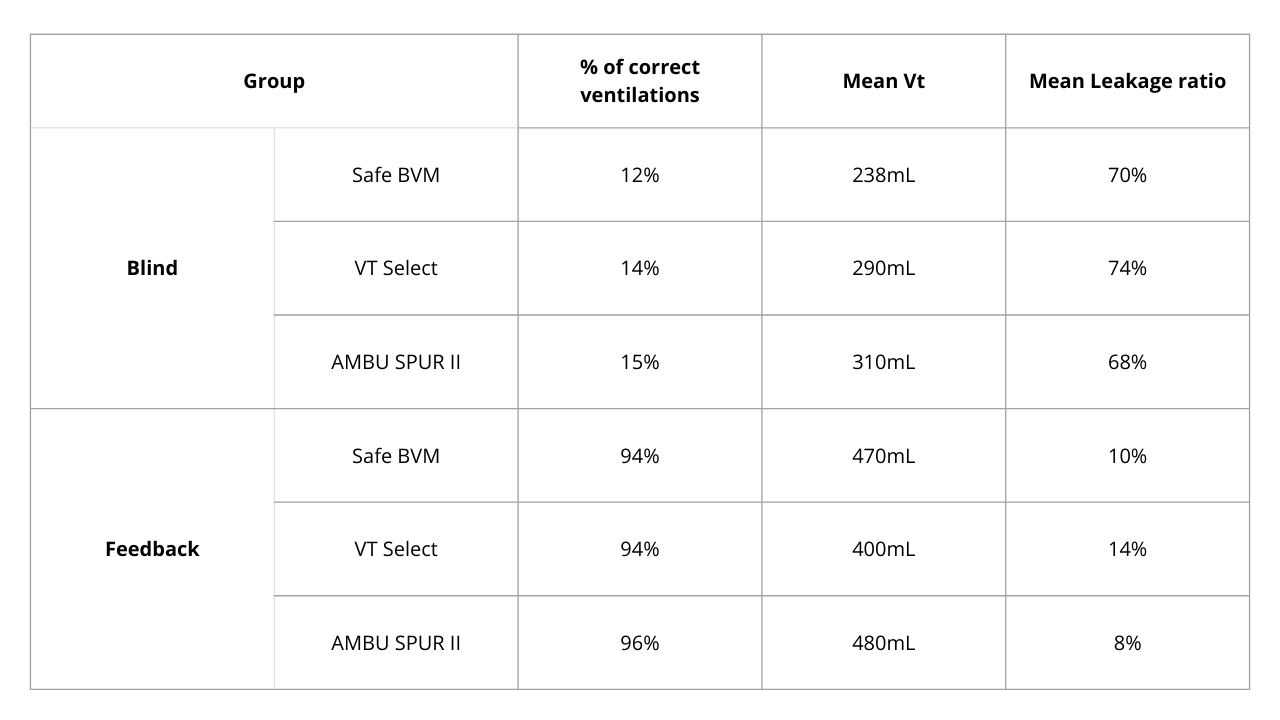
These findings demonstrate that, regardless of the ventilation device used, ventilation without feedback rarely complies with guidelines. Only real-time physiological feedback enables consistent guideline adherence.
Conclusion: turning subjective skill into controlled science
Manual ventilation without real-time feedback is not clinical control—it is guesswork. Decades of device innovation have failed to solve the core problem: the absence of real-time feedback.
This article from Bob Page and the Manual Ventilation Academy clearly demonstrates that the quality of ventilation does not depend primarily on the bag, the mask, or the device—it depends on having access real-time feedback devices like EOlife X.
EOlife X transforms manual ventilation from a subjective skill into a controlled intervention. It improves accuracy, consistency, learning speed, and guideline adherence across all configurations.
In modern resuscitation, the message is clear: bags don’t save breaths—feedback does.

Are you interested in EOlife X to improve your CPR training ?
Learn more
Reference :
https://www.jems.com/patient-care/making-the-case-for-high-performance-ventilation/